


Fall risk
An increased risk of falling for a client, such as Mr Albai, needs to be discussed. Before you start preventative interventions, you must first check whether the client recognizes the increased risk and is motivated to do something about is. See Step 3 of Buurman’s Pyramid. A specialised nurse can start further diagnostics to determine the causes and risk factors of falls.
During a fall-risk evaluation, the risks of falls are examined from several perspectives, such as mobility, balance, dizziness, vision, incontinence, fear of falling, cognition, mood, medication and home/environment. A fall-risk evaluation consists of:
- History of the client
- Physical examination
- History of the risk factors
- Research into mobility
- Investigating the home for fall hazards using a checklist
Multiple causes of the fall risk are tackled in collaboration with multiple disciplines. It is therefore important cooperate with other professionals. A first step is to refer the client to a specialized/HBO vpk for a fall-risk evaluation. Orthostatic hypotension can be measured in a fixed manner. The results can be immediately passed on to the specialized nurse.
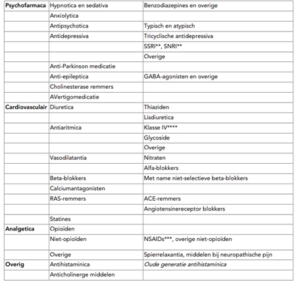
Medications that can increase the risk of falls include:
Other factors that may increase the risk of falling include a previous fall, fear of falling, confusion/delirium, dizziness, Parkinson’s disease, cognitive impairment and visual impairment
Bron:
Federatie Medisch Specialisten. Preventie van valincidenten bij ouderen. Preventie Van Valincidenten Bij Ouderen.pdf
Valrisicobeoordeling ouderen in verpleeghuis – Richtlijn – Richtlijnendatabase
http://www.fysiotherapielindenholt.nl/Draaiboek_screening_valpreventie_DEF.pdf. zie bijlage 2
Bleijenberg (2017) Toolkit kwetsbare ouderen. Bohn Stafleu van Loghum.
Larue A. in : Bakker T., Habes V., Quist, G., Van der Sande, J., Van de Vrie, W. (2019) Klinisch redeneren bij ouderen. Functiebehoud in levensloopperspectief. Bohn Stafleu van Loghum.